
Is My Child Allergic to This Medicine? How to Tell the Difference Between a Medication Allergy and a Side Effect


I'm a parent, and deciding whether to start my children on medication is always stressful! I'm an overthinker, and I think many moms are these days. Side effects and allergies are always top of mind.
Worrying about drug allergies and side effects is... just one more thing to worry about!
If your child has started a new medicine and:
- A rash appears
- They develop diarrhea
- Their bowel movements are funny colors
- They are hyper
- A stomachache or vomiting occurs
It is normal to panic and think:
“Is my child allergic to this medicine?”
Before your brain jumps straight to “allergy,” take a breath. If your child looks and feels well, many of these symptoms are more likely to be a medication side effect or an unrelated part of the illness.
Many medications cause expected side effects that can look alarming and may certainly be unpleasant, but they are not necessarily true allergic reactions.
This guide explains the difference between a medication allergy and a side effect, reviews several common medication reactions in children, and provides guidance about when to call the doctor or seek emergency care.
Medication Allergy vs. Side Effect: A Quick Parent Guide
These are some common medication side effects and possible signs of an allergic reaction. When in doubt, contact your pediatrician or pharmacist.
| If Your Child Has... | It May Be... | What Should You Do? |
|---|---|---|
| Mild diarrhea after starting an antibiotic | Common side effect | Encourage fluids and contact your pediatrician if it becomes severe, persistent, bloody, or is accompanied by signs of dehydration. |
| A flat pink rash several days after starting amoxicillin | Often a low risk medication related rash rather than an immediate allergy | Contact your pediatrician before giving the next dose or assuming your child has a permanent allergy. |
| Red or reddish orange stool while taking cefdinir | Expected medication related color change | This is usually harmless, especially when cefdinir is taken with iron. Contact your pediatrician if you suspect actual blood. |
| Shakiness or temporary hyperactivity after albuterol | Common side effect | These effects usually improve as the medication wears off. Call the pediatrician if they are severe or very bothersome. |
| Hives, facial swelling, wheezing, or trouble breathing | Possible allergic reaction | Seek immediate medical attention. Call 911 for trouble breathing, significant swelling, or signs of anaphylaxis. |
What Is a Medication Allergy?
A medication allergy is an adverse reaction caused by the immune system. This is different from a predictable side effect, such as diarrhea from an antibiotic or shakiness after albuterol.
There are different types of allergic reactions, and they can range from mild to life-threatening. Some reactions also resemble allergies but occur through other mechanisms, so the exact cause cannot always be determined from symptoms alone.
Symptoms of a medication allergy may include:
- Hives
- Facial swelling
- Lip or tongue swelling
- Wheezing
- Difficulty breathing
- Severe rash
- Anaphylaxis
- Sudden or repetitive vomiting
Timing also matters. Immediate allergic reactions often occur within minutes to several hours after a dose and may involve hives, swelling, wheezing, vomiting, or anaphylaxis.
Delayed immune reactions may appear days later. These can range from a mild rash to rare but serious skin or organ reactions.
Any severe or concerning reaction should be evaluated immediately by a healthcare professional.
For trouble breathing, anaphylaxis, or swelling of the face, lips, or tongue, call 911 or seek emergency care.
If your child has been prescribed an epinephrine auto-injector for this type of reaction, give it immediately according to their allergy action plan, then call 911. Do not delay epinephrine while waiting to see whether symptoms improve.
Seek urgent medical evaluation for a rash accompanied by:
- Blistering or peeling skin
- Sores in the mouth or around the eyes
- Skin pain
- Fever
- Facial swelling
- Unusual bruising
- Joint swelling
- A child who appears very sick
Not Every Rash Means an Allergy
This is one of the trickiest “is it an allergy or a side effect?” questions that parents and healthcare providers encounter.
It is always alarming to see a rash on your child, especially if they have just started a new medication.
However, children can develop rashes when they are sick, especially with viral illnesses. Kids get rashes sometimes for no apparent reason at all! If a rash appears after starting a medication, the medication may not actually be the cause.
This is particularly common with antibiotics. It is possible for kids to be sick with more than one bug at a time, meaning they could be fighting off a virus plus whatever bacterial infection necessitated the antibiotic.
A rash may be related to:
- The underlying infection
- A separate viral illness
- The medication
- An interaction between the medication and the illness
- A true immune-mediated (i.e., allergic) medication reaction
A mild rash does not automatically mean that your child has a dangerous drug allergy. However, the rash's appearance when it started, whether it is changing, and whether your child has other symptoms all matter.
Contact your pediatrician for guidance before giving the next dose if your child develops a new rash while taking medication.
How can you tell hives from a common medication rash?
Hives are typically raised, itchy welts. They may move around the body, disappear from one location, and reappear somewhere else. Individual spots often change shape or location over several hours.
Hives can be very uncomfortable. A common mild rash is usually not too bothersome.
A common delayed medication-related rash is more likely to:
- Appear flat or slightly raised
- Look pink or red
- Remain in the same general locations
- Develop after several days of treatment
- Occurs without facial swelling or breathing difficulty
These descriptions can help, but they are not diagnostic. Take clear photos of the rash and contact your pediatrician for help.
My Child Developed a Rash After Amoxicillin. Is It an Allergy?
Ahhh, the amoxicillin rash.
Amoxicillin is commonly used in children for treating illnesses like ear infections and strep throat. Rashes in this setting are also common. Children taking amoxicillin may develop:
- Flat pink rashes
- Blotchy rashes
- Widespread spots
- A rash that appears several days into treatment
These rashes are often delayed, may not be particularly itchy, and may occur while a child is also fighting a viral infection.
A mild, flat rash that appears several days into treatment may be related to the infection, a concurrent viral illness, the medication, or a combination of factors.
Many of these rashes do not represent a dangerous immediate penicillin allergy. However, it is not always possible to determine the cause based on appearance alone!
If the rash is mild, not worsening quickly, not "moving" around, and not otherwise bothering your child, it may be a low-risk rash rather than an immediate allergic reaction.
Contact the prescriber before giving the next dose of amoxicillin. They can review the timing, appearance, other symptoms, and your child's medical history and advise you whether to continue the medication.
This is an example of an amoxicillin rash that DID end up being diagnosed as an allergy. It worsened quickly and became many large moving hives :(

What Does a True Amoxicillin Allergy Look Like?
While mild rashes during amoxicillin treatment are common, amoxicillin can also cause a true allergic reaction.
Possible signs of an immediate allergic reaction include:
- Hives
- Facial swelling
- Lip or tongue swelling
- Difficulty breathing
- Wheezing
- Sudden repetitive vomiting
- Dizziness, fainting, or unusual limpness
- Symptoms that begin within minutes to several hours after a dose
Immediate allergic reactions may occur early in a treatment course, particularly if a child has previously been exposed to amoxicillin, penicillin, or a related medication.
If your child has emergency signs of anaphylaxis, such as trouble breathing, significant swelling, fainting, or rapidly worsening symptoms, call 911 or seek emergency care immediately.
Delayed allergic reactions can also occur. Contact your pediatrician promptly for a rash accompanied by fever, joint pain, facial swelling, blistering, skin peeling, mouth sores, or a child who appears very sick.
Is My Child Allergic to Amoxicillin?
Because reactions can vary, families should always discuss a new rash or suspected reaction with their pediatrician before permanently labeling a child as allergic to amoxicillin.
Your child's doctor can help determine whether a rash during or around the time of amoxicillin use represents:
- A likely immediate allergy
- A low-risk delayed rash
- A medication side effect
- A rash from the illness itself
- A reaction that requires evaluation by an allergy specialist
Amoxicillin is a useful drug. If your child is not actually allergic, you do not want to unnecessarily limit their use later!
Your pediatrician or allergy specialist may recommend a formal allergy evaluation or a supervised oral amoxicillin challenge.
An oral medication challenge involves giving carefully measured doses under medical supervision while monitoring for a reaction. Parents should never test a suspected amoxicillin allergy by giving a dose at home.
Children with a history of blistering rashes, peeling skin, mouth sores, organ injury, severe joint symptoms, or another serious delayed reaction may require a different type of evaluation and are not usually candidates for a routine oral challenge.
My Child Has Diarrhea While Taking Augmentin. Is That an Allergy?
Augmentin, also known as amoxicillin clavulanate, commonly causes diarrhea and stomach upset.
Antibiotics can alter the normal bacteria in the gastrointestinal tract, and the clavulanate component of Augmentin is particularly prone to causing gastrointestinal intolerance.
Augmentin is unfortunately really good at this.
Diarrhea from Augmentin is a known side effect. When it occurs in a child taking the medication, it is usually considered a side effect rather than an allergic reaction.
Giving Augmentin at the start of a meal may improve stomach tolerance, unless the prescriber or product instructions say otherwise.
Call your pediatrician if the diarrhea becomes:
- Severe
- Bloody
- Very frequent or watery
- Persistent
- Associated with significant stomach pain
- Associated with fever
- Associated with signs of dehydration
- Present after the antibiotic course has ended
Routine antibiotic-related diarrhea is much more common than a serious intestinal infection. However, significant or persistent diarrhea should be evaluated.
My Child's Stool Turned Red While Taking Cefdinir. Should I Worry?
This one surprises parents! It is super alarming to wipe your child's bum and see red in the stool!
Cefdinir, commonly used in children for ear infections and other bacterial infections, can interact with iron in the gastrointestinal tract.
Kids may get iron from:
- Infant formula
- Fortified foods
- Vitamins
- Iron supplements
Cefdinir and iron can form a reddish compound that temporarily causes stool to appear red, reddish orange, or brick colored.
Although it can look scary, this is usually a harmless medication-related color change rather than an allergic reaction or internal bleeding.
Iron supplements may need to be separated from cefdinir by at least two hours. However, cefdinir can generally be given with iron-fortified infant formula. Follow the instructions on your pharmacist's label or medication label.
If you suspect actual blood, or if your child also has severe pain, significant diarrhea, weakness, or other concerning symptoms, seek medical care.
My Child Became Hyper After Using Albuterol. Is That Normal?
Yes.
Albuterol stimulates beta-2 receptors to relax the smooth muscle in the airways. It may also cause temporary effects elsewhere in the body.
Albuterol commonly causes:
- Shakiness
- Jitteriness
- Nervousness
- Restlessness
- Temporary hyperactivity
- A faster heart rate
- Difficulty settling down or sleeping
These are expected side effects of albuterol, and they usually improve as the dose wears off over the next several hours.
Some children are barely affected and do not even notice the stimulating effects. Others seem ready to climb the walls of the playroom, run a 5K, and start a small business.
If the side effects are very bothersome, contact your pediatrician. They can confirm that the dose and administration technique are correct and determine whether any changes to the treatment plan are appropriate.
Seek prompt medical advice if your child develops:
- Chest pain
- Fainting
- A severe or persistent racing heart
- Worsening breathing
- Symptoms that are not improving after albuterol
- A need for albuterol more often than prescribed
Why Did Benadryl Make My Child More Hyper?
Benadryl is NOT my favorite routine allergy medicine for children.
Newer antihistamines are usually preferred for everyday allergy symptoms because they tend to last longer and cause less sedation. Diphenhydramine still has specific uses, so follow your pediatrician's recommendation when it has been advised for your child.
Ironically, medications that make adults sleepy can sometimes have the opposite effect in children! Like bouncing off the walls and zigzagging around the room type of opposite. 😦
This is called a paradoxical reaction.
Some children experience paradoxical hyperactivity after taking:
- Benadryl, also called diphenhydramine
- Other first-generation antihistamines
Instead of becoming sleepy, they may become:
- Hyperactive
- Emotional
- Restless
- Excitable
- Irritable
Although surprising and sometimes very annoying, this is considered a side effect of the medication rather than an allergic reaction.
Do not use diphenhydramine simply to make a child sleepy. Ask your pediatrician or pharmacist whether it is appropriate for your child's age and symptoms.
Can Steroids Cause Mood Changes?
Yes.
My daughter had to take a long course of prednisone once, and I swear she had “roid rage.”
Medications such as prednisone, prednisolone, or dexamethasone may cause temporary side effects such as:
- Irritability
- Mood swings
- Increased energy
- Difficulty sleeping
- Increased appetite
- Emotional changes
These changes can feel dramatic and uncomfortable for kids and families, but they are recognized steroid side effects and are not typically signs of an allergy.
When a steroid is prescribed once daily, giving it in the morning and with food may help reduce sleep disruption and stomach upset.
However, follow the prescription directions if the medication is scheduled more than once daily or your child's healthcare provider gives different instructions.
Contact the prescriber if mood or behavioral changes become severe, unsafe, or difficult to manage.
Can Medications Cause Sun Sensitivity?
Yup!
Some medications can make the skin more likely to burn or become irritated in sunlight. This is often called medication-related photosensitivity or sun sensitivity.
Examples of medications used in children and teens include:
- Doxycycline
- Isotretinoin
- Topical retinoids such as tretinoin
Children taking these medications may:
- Burn more easily
- Develop redness more quickly
- Experience skin irritation
- Develop an exaggerated sun reaction
So uncomfortable!
This type of reaction is different from a medication allergy.
Use broad-spectrum sunscreen, protective clothing, shade, and the medication-specific precautions recommended by your child's prescriber.
Is an Upset Stomach From Antibiotics an Allergy?
Not usually.
Unfortunately, many antibiotics commonly cause:
- Mild nausea
- Mild stomach pain
- Diarrhea
- Reduced appetite
These symptoms alone usually suggest medication side effects rather than an allergic reaction.
Vomiting by itself is more often caused by illness, medication irritation, or another side effect than by an allergy.
However, sudden or repetitive vomiting soon after a dose can be part of an allergic reaction, particularly when it occurs with:
- Hives
- Facial swelling
- Lip or tongue swelling
- Coughing
- Wheezing
- Difficulty breathing
- Dizziness
- Fainting
- Pallor
- Unusual sleepiness or limpness
Anaphylaxis can occasionally occur without obvious skin symptoms.
If your child develops sudden repetitive vomiting shortly after a medication dose, especially with any other concerning symptoms, seek urgent medical advice.
For regular tummy troubles, read the medication instructions or contact your pharmacist or doctor. Taking the medication with food may help when the specific medication can safely be taken with food.

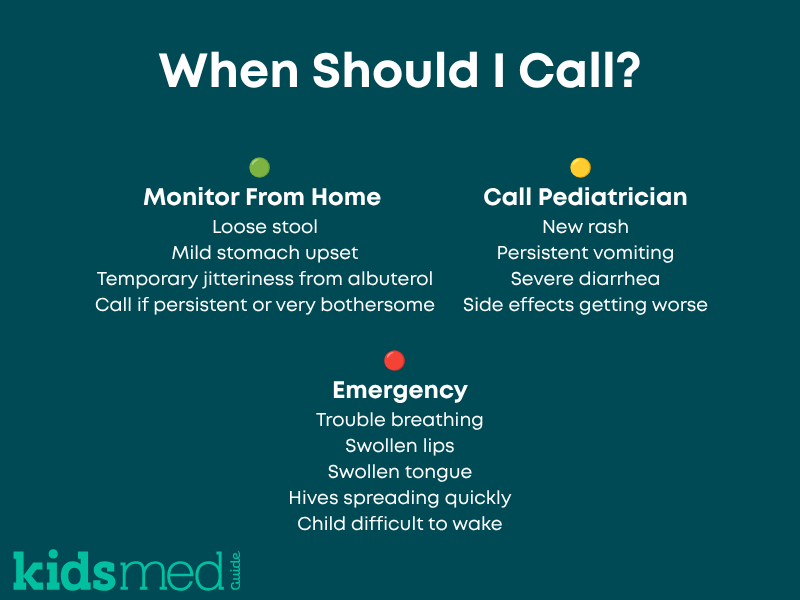
What Should Parents Do if They Think Their Child Is Having a Medication Reaction?
First, look at your child rather than focusing only on the symptom.
Ask yourself:
- Are they breathing comfortably?
- Are they alert and responding normally?
- Is there facial, lip, or tongue swelling?
- Is the rash spreading quickly?
- Are there hives?
- Are they repeatedly vomiting?
- Do they have blistering, skin pain, or mouth sores?
- Do they look very sick?
If your child's symptoms are mild and they look well and comfortable:
- Contact your pediatrician or pharmacist for guidance.
- Take clear photos of any rash.
- Write down when the symptoms began.
- Record when the medication was given.
- Note how long after the dose the reaction started.
- Write down any foods, supplements, or other medicines taken at the same time.
- Pay attention to whether the rash is raised, flat, itchy, painful, moving, or staying in one place.
If the symptom could represent an allergic reaction, especially a new rash, hives, swelling, or repeated vomiting, contact the prescriber before giving another dose.
For a familiar, mild side effect such as loose stool or temporary jitteriness, follow the existing treatment plan and contact the prescriber if symptoms are significant, worsening, or difficult to manage.
If your child develops signs of a serious allergic reaction, call 911 or seek emergency medical care immediately.
Serious symptoms may include:
- Hives that spread rapidly
- Facial, lip, or tongue swelling
- Difficulty breathing
- Wheezing
- Fainting or unusual limpness
- Severe or repetitive vomiting
- A severe blistering or peeling rash
- Signs of anaphylaxis
How Do Healthcare Providers Evaluate a Possible Medication Allergy?
Healthcare providers consider much more than whether a symptom happened while a child was taking a medication.
They may ask:
- Which medication was given?
- Why was the medication prescribed?
- How many doses had the child received?
- How long after the dose did the symptoms begin?
- What did the rash look like?
- Was it raised, flat, itchy, painful, blistering, or peeling?
- Did the rash move around or remain in one place?
- Was there swelling, wheezing, vomiting, fainting, fever, or joint pain?
- Had the child taken the medication before?
- What happened after the medication was stopped?
- Has the child taken the same or a related medication since then?
Photos are incredibly helpful because many rashes improve or disappear before the child is seen by a clinician.
Depending on the reaction, the pediatrician may recommend avoiding the medication, seeing an allergist, undergoing allergy testing, or completing a supervised oral medication challenge.
Why Incorrect Allergy Labels Matter
Once a medication allergy is added to a child's medical record, it often remains there for many years.
This is not ideal if it's not correct!
An incorrect medication allergy label may:
- Limit future treatment options
- Lead to broader spectrum antibiotic use
- Increase healthcare costs
- Increase the risk of side effects from alternative medications
- Contribute to antibiotic resistance
- Result in the use of medications that are less effective or less convenient
We do not want to take away a whole class of useful drugs if there is no need to.
Allergy specialists may recommend a formal evaluation when the reaction history is unclear or appears to be low risk.
However, a medication allergy should never be removed from the medical record based only on a parent's guess. Delabeling should occur after appropriate review and, when needed, supervised testing or a medication challenge.
The Bottom Line
Many medication reactions, including amoxicillin rashes, Augmentin diarrhea, cefdinir-related red stool, albuterol shakiness, Benadryl hyperactivity, and steroid mood changes, are expected side effects or medication-related effects rather than true allergies.
However, it is not always possible to determine the cause of a reaction based on one symptom alone.
The timing, appearance, severity, and presence of other symptoms all matter.
Talk with your pediatrician or pharmacist if your child experiences a reaction to a medication. They can help determine whether it is:
- A known side effect
- A possible allergy
- A symptom of the underlying illness
- A reaction that requires further evaluation
If your child is diagnosed with a medication allergy, make sure it is documented in their medical record and shared with all healthcare providers.
If a previous allergy label is questioned, ask whether your child may benefit from evaluation by an allergy specialist.
Frequently Asked Questions
Does a rash from amoxicillin always mean my child is allergic?
No. A rash during amoxicillin treatment may be related to the medication, the underlying infection, a viral illness, or a combination of factors.
Many mild, delayed rashes do not represent a dangerous immediate penicillin allergy. However, contact your pediatrician before giving the next dose so they can evaluate the appearance, timing, and other symptoms.
Is diarrhea from antibiotics an allergic reaction?
Usually not. Mild diarrhea is a common side effect of many antibiotics.
However, severe, bloody, very frequent, or persistent diarrhea should be evaluated by a healthcare provider, especially if it is accompanied by fever, significant pain, or signs of dehydration.
Why did cefdinir turn my child's stool red?
Cefdinir can interact with iron in the gastrointestinal tract and temporarily cause reddish or orange red stool.
Iron may come from supplements, vitamins, formula, or fortified foods. This color change is usually harmless.
Contact your pediatrician if you are unsure whether the discoloration could be blood.
Can albuterol make kids hyper?
Yes. Albuterol commonly causes temporary shakiness, jitteriness, nervousness, a faster heart rate, or extra energy.
These are expected side effects rather than signs of an allergy. They usually improve as the medication wears off.
What symptoms suggest a medication allergy?
Symptoms such as hives, facial swelling, lip or tongue swelling, wheezing, difficulty breathing, sudden repetitive vomiting, fainting, or anaphylaxis may indicate an immediate allergic reaction.
Delayed allergic reactions may cause a rash several days later. Seek urgent care for blistering, peeling skin, mouth sores, skin pain, fever, facial swelling, or a child who appears very sick.
Should I stop my child's medication if they develop a mild rash?
It depends on the medication, the appearance of the rash, when it began, and whether your child has other symptoms.
If your child develops a new rash while taking medication, contact the pediatrician before giving the next dose. Call 911 for trouble breathing, facial or tongue swelling, fainting, or other signs of anaphylaxis.
Can a medication allergy appear after several days?
Yes. Some medication allergies occur within minutes to hours, while delayed reactions can appear several days or even weeks after treatment begins.
The timing of the symptoms helps healthcare providers determine what type of reaction may have occurred.
Can my child be tested for an amoxicillin allergy?
Yes. Depending on the original reaction, an allergist or other qualified healthcare professional may recommend allergy testing or a supervised oral amoxicillin challenge.
A suspected allergy should never be tested by giving your child amoxicillin at home.
References
5ml solution. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=e8450607-a68c-4729-e053-2995a90a2238
A Parent’s Guide to Over-the-Counter Medicines for Children. (2026, July 6). HealthyChildren.Org. https://www.healthychildren.org/english/safety-prevention/at-home/medication-safety/pages/choosing-over-the-counter-medicines-for-your-child.aspx
Allergies in Children: Causes, Symptoms, Types & What Parents Can Do. (2026, April 21). HealthyChildren.Org. https://www.healthychildren.org/English/health-issues/conditions/allergies-asthma/Pages/Allergy-Causes.aspx
CLAV POT ORAL SUSP powder, for suspension. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=e5bd9918-b073-c50b-e053-2a95a90aaeb7
DailyMed—ALBUTEROL- albuterol sulfate aerosol, metered. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=fd0389e0-3713-42e0-8ef2-3bb97676fded
DailyMed—AMOXICILLIN- amoxicillin powder, for suspension for suspension. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=b42baeeb-16b6-4a85-aa94-c40532925941
DailyMed—CEFDINIR powder, for suspension. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=efb5a975-75ec-46e1-ba84-f68d0b9bf36f
DailyMed—DEXAMETHASONE INTENSOL solution, concentrate. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=a817ab46-54ec-4e3f-886b-04ce6ac1caf9
DailyMed—DOXYCYCLINE capsule. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=a894f4be-19e5-4785-8d0b-5e0d5626300e
DailyMed—ISOTRETINOIN capsule. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=1cf11710-f966-4529-8e08-02175f588bca
DailyMed—PREDNISOLONE- prednisolone oral solution solution. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=b079834f-9aa3-4db9-bd53-de28e8f81c04
DailyMed—PREDNISONE TABLETS, USP, 5 MG- prednisone tablet. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=419058f7-7f30-41a1-964b-8eaa69290dea
DailyMed—TRETINOIN CREAM- Tretinoin cream. (n.d.). Retrieved July 13, 2026, from https://www.dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=745cc3ce-60b4-4479-a055-316817567949
Drug allergy: A 2022 practice parameter update—Journal of Allergy and Clinical Immunology. (n.d.). Retrieved July 13, 2026, from https://www.jacionline.org/article/S0091-6749(22)01186-1/fulltext
Drug allergy—Symptoms and causes. (n.d.). Mayo Clinic. Retrieved July 13, 2026, from https://www.mayoclinic.org/diseases-conditions/drug-allergy/symptoms-causes/syc-20371835
Lim, P. P. C., Moore, L. N., Minich, N. M., Wessell, K. R., & Desai, A. P. (2024). Inpatient allergy delabeling of pediatric patients with low-risk penicillin allergy status through direct oral amoxicillin challenge. Allergy and Asthma Proceedings, 45(1), 61–69. https://doi.org/10.2500/aap.2024.45.230069
Medication Side Effects & Reactions. (2016, May 13). HealthyChildren.Org. https://www.healthychildren.org/English/safety-prevention/at-home/medication-safety/Pages/Medication-Side-Effects.aspx
Medications and Drug Allergic Reactions | AAAAI. (n.d.). Retrieved July 13, 2026, from https://www.aaaai.org/tools-for-the-public/conditions-library/allergies/medications-and-drug-allergic-reactions
Symptomviewer. (2017, June 24). HealthyChildren.Org. https://www.healthychildren.org/English/tips-tools/symptom-checker/Pages/symptomviewer.aspx
Trickett, J., & Chambliss, J. (2023). Delabeling Penicillin Allergy in A Pediatric Primary Care Clinic. Pediatrics, 152(Supplement 3), S16. https://doi.org/10.1542/peds.2023-064344F
Wheatley, L. M., Plaut, M., Schwaninger, J. M., Banerji, A., Castells, M., Finkelman, F. D., Gleich, G. J., Guttman-Yassky, E., Mallal, S. A. K., Naisbitt, D. J., Ostrov, D. A., Phillips, E. J., Pichler, W. J., Platts-Mills, T. A. E., Roujeau, J.-C., Schwartz, L. B., & Trepanier, L. A. (2015). Report from the National Institute of Allergy and Infectious Diseases workshop on drug allergy. Journal of Allergy and Clinical Immunology, 136(2), 262-271.e2. https://doi.org/10.1016/j.jaci.2015.05.027



